![]()
![]()
Treatment options
 Together we can make a world where cancer no longer means living with fear, without hope, or worse
Together we can make a world where cancer no longer means living with fear, without hope, or worse
Cancer pain becomes more frequent as the malignancy progresses, with one-third reporting pain at the time of diagnosis and 60–80% of patients with advanced cancer.
Tumor growth and metastasis can cause pain in any organ. The skeleton is the most common site of cancer.
Mechanisms by which cancer causes pain include, tissue damage and inflammation, nerve compression and infiltration, increased intracranial pressure, obstruction of hollow organs and distension of capsules surrounding internal organs such as the liver and spleen.
Pain reported by cancer patients can be categorized as nociceptive somatic, nociceptive visceral, neuropathic and psychogenic. Pain secondary to infiltration of bone is classified as nociceptive somatic. Nerve root compression from tumors manifests itself as neuropathic pain
Pain could be classified as originating from nociceptors of the bone (35%), soft tissue (45%) or visceral structures (33%) neuropathic origin (34%).
In most patients, pain syndromes were located in the lower back (36%), abdominal region (27%), thoracic region (23%), lower limbs (21%), head (17%) and pelvic region (15%)
Psychiatric Complications
Psychologic symptoms such as worrying, nervousness, lack of energy, insomnia, and sadness are the most prevalent and distressing symptoms encountered in this population.
Neuropsychiatric symptoms and syndromes, such as mood disorders (i.e., depression), cognitive impairment disorders (i.e., delirium), anxiety, insomnia, and suicidal ideation have a crucial role in management of patients with advanced disease. Pain is a common problem for cancer patients, with approximately 70% of patients experiencing severe pain at some point in the course of their illness.
DELIRIUM AND COGNITIVE IMPAIRMENT DISORDERS
Delirium is extremely common in cancer patients, particularly those with advanced disease. In cancer inpatients, the prevalence of cognitive impairment is 44%, with the prevalence rising to 62.1% just before death. The clinical features of delirium include a variety of neuropsychiatric symptoms that are also common to other psychiatric disorders such as depression, dementia, and psychosis
MAJOR DEPRESSIVE DISORDER
An study reported that approximately 50% of patients with malignancies experience some kind of psychiatric disorder, adjustment disorders and major depression are the most common psychiatric disorders.
Peripheral Neuropathy Due to Chemotherapy and Radiation Therapy
Chemotherapy agents have been used for many years in the treatment of different solid and nonsolid malignant tumors. Chemotherapy induced side effect includes, pain, fatigue, depression, nausea, vomiting, diarrhea, constipation, cardiac arrhythmias, vascular and pulmonary toxicity, skin changes, mucositis, and sensory-motor disturbances.
RADIATION-INDUCED PERIPHERAL NEUROPATHIES
Patients with neuropathies can present with many different signs and symptoms, depending on the nerves affected. With radiation delivered close to the spinal cord where the nerve roots emerge, the patient may experience radiculopathies. At the level of the cervical and lumbar spine, the patient often complains of back pain, headaches, extremity pain, numbness, paresthesia, and weakness. Radiation to the thoracic area may cause noncardiac chest pain and abdominal pain.
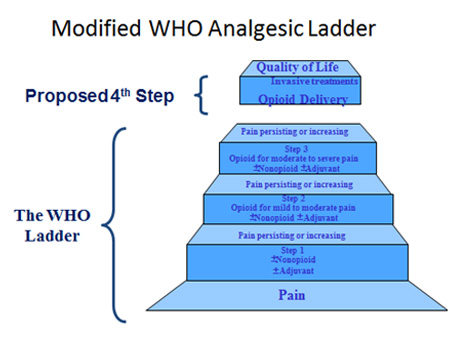 Treatment options
Treatment optionsNon-Opioids : NSAIDS Acetaminophen
Weak opioids : Tramadol
Strong opioids
Morphine
Transdermal fentanyl
Transdermal Buprenorphine
Adjuvants
| Indication | Drugs |
| Neuropathic pain | Amitriptyline, gabapentine, clonazepam, dexamethasone |
| Neuropathic pain unresponsive to above | Ketamine |
| Bowel obstruction | Hyoscine butylbromide, octreotide |
| Bone pain | Pamidronate, zolendronate, dexamethasone |
| Cerebral edema, headache | Dexamethasone |
| Painful wound | Antibiotic |
| Liver capsule pain | Dexamethasone |
| Gastritis | PPI, |
| Gastric distension | Metaclopromide |
| Esophageal spasm | nifedipine |
| Intestinal colic | Hyoscine butylbromide |
Copyright © 2026 Kathmandu Pain Management Center. All Right Reserved
Design by: webdesigninnepal.com



